Looking for a Silver Lining
Plenty of dark clouds around

These posts examine modern psychiatry from a critical point of view. Unfortunately, mainstream psychiatrists usually react badly to any sort of critical analysis of their activities, labelling critics as “anti-psychiatry,” whatever that is. Regardless, criticism is an integral part of any scientific field and psychiatry is no different. As it emerges, there is a lot to be critical about.
If you like what you read, please click the “like” button at the bottom of the text, it helps spread the posts to new readers. If you want to comment, please use the link at the end rather than email me as they get lost and nobody sees them.
****
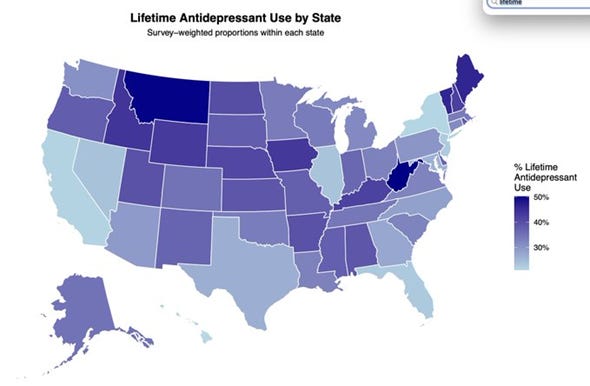
What with everything going on in the world today, people seem to have more important things to worry about than mental health but Mr RFK Jr, US Secretery for Health, hasn’t been asleep on the job. In the original “Make America Healthy Again” plan from last year, the goal was to reduce prescription rates of psychiatric drugs, mainly in children but also in adults. Predictably, the psychiatric establishment reacted badly because psychiatry as a discipline is now based almost entirely on the single notion that “mental disorder is brain disorder.” This separates and distinguishes psychiatrists from all other fields. In particular, practically all research and treatment flows from this one point, so the idea that people can get by without drugs threatens their very comfortable (and intellectually undemanding) living. However, they’d better get used to it because the next step, deprescribing, is on the way. In the MAHA program, deprescribing is directed mainly at children but also at antidepressants in adults. A recent survey quoted by a psychiatrist says over 16% of all American adults are taking these drugs daily, and about 34% have taken them at some stage in life:
A recent representative survey of ~30,000 US adults examined antidepressant and psychotherapy use plus attitudes toward regulation. As in prior studies, 16.6 % of adults (1 in 6) reported current antidepressant use. But the study also reported the less commonly examined lifetime prevalence: 33.9 %, 1 in 3 Americans have ever used prescription antidepressants. The prevalence was higher in females at 42.5 % (≈ 1 in 2.35). Lifetime use was a majority of adults in: Nonbinary individuals: 63.1%; West Virginia (50.2%) and almost Montana (50.0%). Lifetime use was >40% in: Idaho, Iowa, Kentucky, Maine, Nebraska, New Hampshire, North Dakota, Vermont, Wyoming. Lifetime use was also >40% in: people without a high school diploma; age group 45-54; and living in rural areas.
Australian figures aren’t quite as bad but they’re heading in the same direction even though, on all counts, antidepressants don’t work. With one person in six taking them, suicide rates should be right down, fewer people on pensions for depression, less time off work, etc. None of this is true. Suicide rates are high and rising, more and more people are on pensions for mental disorder and depression is listed as a major cause of “burden of illness” internationally. That’s exactly the opposite of what they should be doing so perhaps it’s time for an official body to ask whether they should be so freely prescribed. Allen Frances, former chair of the DSM-IV committee and largely responsible for the explosion in psychiatric diagnoses in children, tweeted:
Miracle of miracles: RFK Jr finally gets something right. Announces new federal effort to reduce ridiculous 16% rate of antidepressant use in US. We need guidelines to stop careless prescribing/encourage careful deprescribing. Great news/great piece.
Three cheers for Mr K, but before everybody gets too excited, DropSite News has some bad news (halfway down page, under “US News”):
Food and Drug Administration officials have blocked publication of several studies supporting the safety of widely used Covid-19 and shingles vaccines in recent months … In October, FDA scientists were directed to withdraw two Covid-19 vaccine safety studies that had been accepted by peer-reviewed journals; in February, top FDA officials declined to sign off on submitting abstracts about Shingrix shingles vaccine studies to a major drug safety conference. Both withdrawn Covid studies—one examining 7.5 million Medicare beneficiaries and another examining 4.2 million vaccine recipients across ages six months to 64 years—found serious side effects to be very rare. The suppressed studies are part of a broader pattern: the CDC’s interim leader canceled a report finding Covid vaccines sharply reduced hospitalizations last winter, and Health Secretary Robert F. Kennedy Jr.’s office previously sought deletion of a vaccine safety summary from the CDC website (May 6th 2026).
That is definitely not worth getting excited about. It’s clear that the Department is ideologically-driven, which is dangerous. It brings to mind another example when a department that should be boringly scientific was taken over by a fanatic, with disastrous results. In the 1920s, after years of war, the newly-formed USSR was in trouble. Vast areas of agricultural land had been damaged in the fighting and there was a shortage of healthy young men (and horses) to work the farms. Undeterred, Stalin pressed ahead with the collectivisation of agriculture, with catastrophic results. In the nation-wide famine in 1932-33, up to 5million people died, especially in Ukraine where it appears to be an engineered attempt at genocide. In persisting with what was clearly a disastrous program, Stalin was swayed by a young and poorly-trained horticulturalist from Ukraine, Trofim Lysenko (1898-1976).
Very early in his career, Lysenko had decided that classic or Mendelian genetics was false and that plants could gain new traits from experience. This was seen as a quick way of developing new crops for difficult climates with poor soil so Lysenko was soon promoted. He used his new power to get rid of well-trained and experienced opponents as “enemies of the people,” replacing them with equally inexperienced or ignorant people who would support him as they owed their jobs to him (and could avoid the military, as well). After Stalin’s death in 1953, Lysenko was protected by the new leader, Khrushchev, who was also Ukrainian and needed all the support he could get. Following the party coup in 1964, Khrushchev was pushed out. Lysenko was quickly accused of pseudoscience and was dismissed from his many posts but it took years for Soviet agricultural sciences to recover from his malign and egocentric influence.
Is RFK Jr in the same league as Trofim Lysenko? He too is absolutely convinced he knows everything he needs to know about a complex scientific field without ever having studied it, as in: “mainstream science has got it wrong; the scientific establishment is more concerned with protecting its privileges than looking after the people; conspiracies about vaccination and health are rife,” etc. Among his many fascinations, Kennedy has recently claimed a link between circumcision and autism, possibly because the infants are given paracetamol (acetaminophen). Most of his ideas are driven by egocentricity: “I know better than anybody,” supported by carefully selected and manipulated “evidence” and constant accusations that anybody who disagrees with him is a bad actor. He appears to be immune to criticism, even from people such as his cousin, Caroline (former ambassador to Australia) who called him a “drug addict and predator.” But this time, he may be backing the right horse. The modern drug industry is built on the idea that people will buy more drugs if they’re scared regularly, similar to how the medieval church scared people to buy indulgences for themselves and their relatives.
Even a broken clock is correct twice a day, and in the rush to improve standards of health, there may have been some overreactions so we need to tread carefully, e.g. Kennedy’s campaign against immunisation. In my childhood, there were children in our small town who died of diphtheria, polio, tetanus, congenital heart disease and other treatable horrors. When the polio immunisation arrived, there was not a word of argument. Every child in the school lined up and got the jab. There were children at school who had had polio, we could all see each day what it did, so there was no nonsense about taking sheep medicine (ivermectin) to prevent it. The world is indeed better off with public immunisation schemes but the question here is: Are we better off with widespread dosing of the population with psychoactive drugs? That’s a totally different question because nobody has ever shown that mental problems and, say, viral infections belong in the same category. Yes, they are afflictions but the question is whether they’re of the same order of being, meaning both the sorts of things that respond to physical treatments. Mainstream psychiatry says: “Yes, all mental disorder is physical in nature so physical treatment is obligatory.” In fact, failing to provide physical treatment can be seen as negligent, with all the complications that flow from that.
The other side of the argument is that there is a highly developed scientific basis to treating infections. We know how ivermectin works on parasites, by blocking neural transmission at the level of glutamate-gated chloride channels, which paralyses then kills the worm. How do we know that intestinal worms have nerves at all? Well, that’s a major part of what science is, the steady accumulation of strongly confirmed conjectures about basic mechanisms [1]. Years ago, somebody put a tiny helminth under a microscope and painstakingly dissected it. Now we know that for dogs, 0.001mg/kg of the animal’s weight is enough ivermectin to kill the worms, that’s just ten millionths of a gram in a 10kg dog. That’s pretty impressive. Psychiatry doesn’t have anything like that because it doesn’t have a basic understanding of its subject matter. This is not academic. For all its potency, does ivermectin have any effect on viruses? No, it works by blocking nerve transmission, especially the type of nerves found in parasitic worms. Humans don’t have that particular neurotransmission so it’s relatively non-toxic for us (but still dangerous) while viruses don’t have nerves at all. That’s why it doesn’t work on Covid, or hantavirus, or the common cold or anything of that nature. Claiming (as Kennedy and Trump do) that ivermectin will work on viruses is a bit like claiming that since I have a single key in my pocket, I can open every door in the world. It’s the wrong mechanism.
Given that, can anybody claim that mental disorders are of the same order of being as using a selective poison to kill bowel infestations? Mainstream psychiatry says they are but they have never offered any evidence to support this position. It is an ideological claim with no factual basis [2, Chap. 2]. In the absence of any valid argument on the nature of mental disorder, mainstream psychiatry and the private drug industry are simply acting as though the debate is settled when, by bluster and stealth, they made sure it never started. What, for example, if mental disorder is caused by a breakdown in the social setting? Take the example of a creature that needs to feel a valued part of a social group in order to feel good and to function properly. Given what we know about it, if one of them is emotionally isolated from its peers, it will start to “break down” in various ways. The so-called breakdown is mediated by the mechanisms of the creature’s physical body yet it is caused by or precipitated by social events, i.e. without just those events, it would not have fallen apart.
Another example: a creature is known to react badly to oppression, with emotional and behavioural disturbances and frequent bursts of violence. That’s its nature, that’s what it’s designed to do, so if it is subject to oppression and reacts violently, is that “mental disorder”? A third creature shows all the features of being “territorial,” i.e. needing to be in familiar surroundings in order to function properly, of acquiring territory, goods and possessions for the purpose of feeling more secure, and of showing controlling and even jealous behaviour over others in its surroundings. If that creature loses its territory, it will show a stereotyped reaction to the loss. And when we have a creature like H. sapiens, which has all three of those features in abundance, and is surrounded by people trying to gain social control, dominance and territory at the expense of others, then there is a case for saying that at least some mental disorder is caused by social factors and ipso facto requires a social remedy. Drugs can have only a marginal role directed at specific, damaging symptoms but they are not curative. So far, RFK Jr is on strong grounds but we can go a step further.
Modern psychiatry is based firmly in the concept of reductionism, the idea that the behaviour and properties of a higher order entity are fully explained by the behaviour and properties of the lower order entities of which it is composed. Therefore, human behaviour is fully explained by knowledge of the brain, hence the reliance on drugs, ECT and so on. Trouble is, this does not apply to informational states: information cannot be reduced to its vehicle. The informational content of a newspaper is not explained by the properties of paper, ink, etc. Information represents a different order of being from the physical universe in that each is controlled by entirely different sets of rules with no points of contact. For example, the rules governing morality are not related to the laws of physics in any way. The biocognitive model says that the human mind is an emergent informational state generated by the brain’s computational capacity. As such, it has its own rules which have nothing to do with physics, no points of contact: if I think of Uluru, my head doesn’t get heavy.
Needless to say, as a rule-governed computational artefact, the mind is totally dependent on the functional integrity of the brain. We take the brain for granted, it always seems to restart itself each morning or after each drinking session but it’s actually functional only within very narrow physiological limits. Outside those limits, it malfunctions but (and it’s an important but) in predictable ways which are distinct from what is deemed “mental disorder.” Personality, of course, is purely informational [3, Chap. 8] so personality disorder is an informational state only and brain chemistry etc. has nothing to do with it, therefore drugs can never work. Trouble is, psychiatry is engaged in a long-term project to reclassify all personality disorder as mental disorder and put people on drugs with terrible side effects, which induce their own “chemical imbalances of the brain” [4, Chaps. 14-16]. So if Kennedy and his minions at the Health Dept. manage to reduce psychiatric drug prescriptions, they’re on solid theoretical grounds: the mind is an informational state, and drugs don’t work on information.
At this stage, we lesser mortals are just spectators to the chaos in the northern hemisphere. Perhaps some good will come from the various obsessions of Trump and Kennedy but it will probably be outweighed by the damage caused by their other projects. Who knows, but if Kennedy ever wants a theoretical basis to reducing overall levels of psychotropic medication, just let him know there’s one written and ready to go [3]. All he has to do is read it but that’s unlikely because he already knows everything.
References:
1. Popper KR (1972). Conjectures and Refutations: the growth of scientific knowledge. London: Routledge.
2. McLaren N (2024). Theories in Psychiatry: building a post-positivist psychiatry. Ann Arbor, MI: Future Psychiatry Press. Amazon.
3. McLaren N (2021): Natural Dualism and Mental Disorder: The biocognitive model for psychiatry. London: Routledge. Amazon
4. McLaren N (2012). The Mind-Body Problem Explained: The Biocognitive Model for Psychiatry. Ann Arbor, MI: Future Psychiatry Press.
****
My critical works are best approached in this order:
The case against mainstream psychiatry:
McLaren N (2024). Theories in Psychiatry: building a post-positivist psychiatry. Ann Arbor, MI: Future Psychiatry Press. Amazon (this also covers a range of modern philosophers, showing that their work cannot be extended to account for mental disorder).
Development and justification of the biocognitive model:
McLaren N (2021): Natural Dualism and Mental Disorder: The biocognitive model for psychiatry. London, Routledge. At Amazon.
Clinical application of the biocognitive model:
McLaren N (2018). Anxiety: The Inside Story. Ann Arbor, MI: Future Psychiatry Press. At Amazon.
Testing the biocognitive model in an unrelated field:
McLaren N (2023): Narcisso-Fascism: The psychopathology of right wing extremism. Ann Arbor, MI: Future Psychiatry Press. At Amazon.
The whole of this work is copyright but may be copied or retransmitted provided the author is acknowledged.
Whilst the Covid vaccines were based on a valid mechanism of action, the companies behind them (Pfizer, Johson and Johnson etc) are still the same as the ones that produce the psychiatric drugs.
Knowing how they act and conduct themselves in their studies to get psych drugs to market, there’s no reason to think they would act much differently with the vaccine (ignoring side effects, statistical manipulation etc).
It was also how people were coerced from companies that you must have the vaccine or lose your job or stranded in countries where they could not leave unless they had an injection, along with the idea that everyone in low risk groups (children, babies) must be vaccinated, that I think contributed towards animosity toward Covid vaccines.
Patrick Hahn provides a deep analysis on this topic in his book, and one case I remember was this one where, given her age, she didn’t seem to be hugely at risk: https://www.bbc.co.uk/news/av/health-57853285
I don’t disagree in principle with vaccinations of course, but the way these companies prove efficacy to bring their psychiatric drugs to market should, at the very least, make one wary of how they prove efficacy for any other drug (especially without standard clinical trials), be it vaccine or not.
The preface and introduction of the Maudsley guide to deprescribing should be required reading for anyone being offered psychotropics. As you say, if people knew how difficult it is to come off them, they would definitely have second thoughts about starting.
It brings to mind a discussion I had with some Americans that I was doing business with who asked my opinion about US intervention in Iraq in 2003. My response was "It's much easier to start a war than finish it". Same with psychotropics.
People should be informed about the probability of weight gain. Data from the drug industry underplays its significance, but my impression is that weight gain is more or less assured, often with catastrophic effect. When an individual is so affected, the impact for them is no longer merely a statistical probability , it's an absolute reality.
Health care is delivered in silos. GPs defer to specialists and aren't inclined to question entrenched processes of decision making that are rooted in myths about a biological model of mental illness.
As I see it, there is cost shifting in three directions from mental health services
1. to GPs to manage metabolic and other consequences of psychotropics
2 to social services that have to contend with many folk who become unemployable
3 to the PBS for drugs that cost- what ? $12000 to $15000 per year per person for drugs that are scarcely better than placebo.
Not to mention the burden upon families and the community.
If people want pills, how about trying placebos first while helping them to get a handle on their well being?
Multiple state and commonwealth governmental reports have described systemic failures of mental health services throughout the country. In South Australia there are attempts to acknowledge and address shortcomings with the introduction of lived experience into policy development and service delivery. This is an area that interests me and there are some "green shoots", albeit under the umbrella of the Mental Health Act.
It might be a crazy idea, but what if people demand support for their health and well being in each of the dimensions suggested. There could be reallocation of resources that would produce much better outcomes? Its political.
What happened in dentistry ( my past life) is that people started to abhor the idea of having their teeth replaced by dentures. Fluoridation came along, which meant that waiting rooms were no longer packed with people needing cavities filled or teeth extracted. Private practitioners then made hygiene the core of their business model, even if it wasn't the main profit centre. Practitioners switched to identifying with the concept of preventive dentistry. The practice of dentistry as it was conceived when I graduated, is now well and truly redundant.
Maybe there are parallels? It's a long game.