DSM6: Old Wine in a Last Century’s Bottle.
Plus ça change, plus c'est la même chose.

These posts examine modern psychiatry from a critical point of view. Unfortunately, mainstream psychiatrists usually react badly to any sort of critical analysis of their activities, labelling critics as “anti-psychiatry,” whatever that is. Regardless, criticism is an integral part of any scientific field and psychiatry is no different. As it emerges, there is a lot to be critical about.
If you like what you read, please click the “like” button at the bottom of the text, it helps spread the posts to new readers. If you want to comment, please use the link at the end rather than email me as they get lost and nobody sees them.
****
Sorry to be the bearer of bad news but the American Psychiatric Association (APA) is gathering its skirts in order to launch another version of its Diagnostic and Statistical Manual of Mental Disorders (DSM) on the world. “What have we done to deserve this?” you sigh, but they need to keep the pot boiling in case people lose interest, not to overlook the rivers of money it generates. The first version was issued in 1952, little more than a rewrite of the US Army’s manual from World War II, which was largely written by psychoanalyst William Menninger and gave it a heavy Freudian bias. The
APA’s DSM continued the tradition over about 130 pages and 106 separate diagnoses. That didn’t matter as nobody took any notice of it. DSM-II arrived in 1968, 134 pages with 182 disorders, prominent among them being homosexuality. This was largely the result of the psychoanalysts, especially Irving Bieber and Charles Socarides, who were convinced to delusional intensity that it was “caused by” early childhood trauma and could be “cured” by psychoanalysis. Socarides more or less devoted his career to this “illness” but his results weren’t so good, with only a third of his patients reporting they had changed their orientation. He was bitterly opposed to the vote in 1973 to remove homosexuality from the list of mental disorders (note that: vote).
By the mid-1970s, psychoanalysis was losing its shine. When it came time to revise DSM-II, none of them wanted to be part of it as they said the entire idea of classifying mental disorder was wrong. However, there were two huge pressures behind the scenes that their lofty disdain couldn’t grasp, the drug and insurance industries. US psychiatry was a house divided. On one side were the vast asylums, known as state hospitals, where huge numbers of patients were simply warehoused and drugged or shocked into silence. The psychiatrists who worked in them were regarded as the lowest form of medical life with no understanding of mental disorder and hundreds of patients to look after, so they spent their lives writing scripts and giving ECT for “biological diseases.” On the other side were the private psychiatrists and academics who were strongly oriented toward Freudian theories and who regarded their state hospital colleagues as little more than vets in charge of herds of drugged cattle.
The job of rewriting the DSM was left to a single group at Washington University, confusingly located in St Louis, Missouri. Most unusually, they were academics who were convinced psychiatry was biological. Over years, they rewrote the entire DSM concept to standardise it – for the benefit of academics but also for the insurance and drug industries. Insurers objected to paying very large sums for apparently endless psychotherapy that seemed to depend more on the psychiatrist’s fancies than any defined scientific standards. Big Pharma, of course, could already see immense financial returns from changing the direction of the lumbering ship of psychiatry. And so, in 1980, DSM-III was born, to great fanfare and self-publicity by the APA. Diagnoses were made by ticking boxes, not by listening to patients ramble on about their unhappy lives. However, it soon became clear that nobody was paying much attention to it, so they made some changes. All the codes were realigned to match the ICD from WHO, and American journals of psychiatry required all authors to use DSM-III. With these in place, it took off. Soon, the ideas behind DSM dominated professions such as nursing, psychology, social work and, importantly, law, insurance and so on.
Very quickly, when talking about the DSM-III, people began using the brain-dead expression, “the bible of psychiatry,” unaware of or unconcerned by two important foundational features. The first was that it was avowedly “atheoretical,” meaning it assumed nothing about the nature of mental disorder. It was purely descriptive, with no explanatory value whatsoever. The second was the idea of mental disorders forming distinct categories with no overlap, either with each other or, more importantly, with normality. Instead of the common sense idea that, say, anxiety varies from the mildest sense of apprehension all the way across to mind-melting terror, they said “ Not so. Normality and mental disorder are different and (crucially) we can tell them apart. All the symptoms of one disorder are unique to just that disorder and can reliably be distinguished.”
Straight away, there was what philosophers politely call a “tension” between these two fundamental points, meaning they don’t make sense. If you say that mental disorder is categorically different from normality, you are automatically saying something about its nature. Just what wasn’t clear but it was some thing, some important point. In fact, the idea of distinct categories of mental disorder only makes sense within a biological framework, where the separate conditions each map down to a distinct and identifiable fault in the genome. That’s the only way it makes sense, and it’s not surprising that, over considerable opposition, this approach was built into the DSM system by committed biological psychiatrists, because that’s how they think. A decade after DSM-III issued, one of the leaders, Samuel Guze, said: “... there is no such thing as a psychiatry which is too biological” [1]. A psychological approach, on the other hand, allows different contributing factors to produce different outcomes, all of which has to be explored. This brings in the concept of non-linear determination, compared with the simple linear concept of causation (mostly) used in the physical sciences.
In turn, the idea of categories is built on a falsehood, that there is no overlap between each other and with normality. Clearly, this is wrong: practically every measure in humans is a matter of degrees, not absolutes: when does high blood pressure become a disease? Even with something as clear-cut as malignancy, there is a blurred borderland between “normal variation” and “diseased” cells. All the cutoff points in the entire DSM are artificial, not helped by the irritating American habit of using the word “marked” to mean “quite a lot, very much, heaps,” etc. Marked means “noted,” as in “a marked man,” i.e. “he has a mark on him.” It is an adjective, not an adverb. Moreover, and all too often, criteria in one diagnosis are simply artfully reworded criteria from another, so it’s a matter of flipping a coin where the patient goes, e.g. “unable to form stable relationships with peers” and “actively avoids intimate involvement with non-family members.” In reality, there’s no difference (see [2] Chap 8 for gripes about DSM-IV; they’re still the same). They make out that DSM is precise and therefore scientific but it’s not, the sloppiness is built in from the beginning. All the revisions since 1980 have only made it worse by encroaching on normality [3] to create new “mental illnesses” where none existed before, e.g. ADHD, ASD, Bipolar II, etc. As a result, DSM-5 has 1120 pages (hardback) and nearly 300 diagnoses with many variants and qualifiers, many of which have metastasized to common speech (but that happened with psychoanalysis as well, people just love to talk about their heads).
None of these problems have been resolved but the new version is on the way, as a recent article shows [4]. Titled Initial Strategy for the Future of DSM, a committee of worthies set out some of the matters to consider, starting with the idea that since DSM-III some 45 years ago, “... knowledge about psychiatric disorders, the psychosocial and cultural impact on them, their treatment, and their biology has evolved tremendously ...” DSM-III was developed “... when there were several conflicting hypotheses about causal mechanisms of mental illness ...” so it was atheoretical, but they wonder if this is still necessary? On second thoughts, it probably is:
One could, of course, defend the decision to make DSM atheoretical even today. Although there is broad agreement in the field that disorders arise from the interplay of neurobiological, developmental, experiential, socioeconomic, cultural, and environmental factors, knowledge about precisely how these factors interact is still evolving. Given that we still do not fully understand the etiology of disorders ... (we’ll probably do nothing bold) [4, p292; emphasis added].
Next, they wondered about the validity of the idea of categories of mental disorder but again were left shaking their heads:
Indeed, the somewhat arbitrary nature of categorical boundaries is one contributor to the extensive overlap in symptoms that we observe in many disorders, the considerable heterogeneity within a given disorder, and the high frequency of comorbidity, which indeed, rather than being the exception, is common in psychiatry ... (p292; emphasis added).
However, the need to do something pushed them to make a choice: “... clinical decision making involves categorical choices among a set of finite options,” meaning: “It’s not our fault, we have boxes to tick.” Other problems include the perpetual dilemma for psychiatry, reliability vs. validity. Validity is when a person correctly identifies something, reliability is when two people agree on what it is. Long ago, the DSM gave up on validity in favour of reliability. It was more important to have psychiatrists agreeing with each other than to be sure that what they were agreeing on was true or correct, just because nobody actually knew. There were no identifiers apart from what the psychiatrists said it was, which leads naturally to their next hurdle, biomarkers. Much as they would like them, psychiatry has no biomarkers. There are no blood tests for depression, no abnormal scans for schizophrenia, no genetic markers for bipolar disorder:
Despite the tremendous progress in our understanding of brain structure and function, this knowledge base is rapidly evolving and remains decidedly incomplete (p293) ... the majority of biological measures, especially biomarkers, are not yet ready to be deployed clinically, other than for Alzheimer’s disease (p297).
Next, they turn to the hoary argument over the scientific status of their diagnostic system:
Another critique is that DSM is not based on empirical science, but rather has been developed through expert consensus ... (However,) the experts base their consensus on empirical data that is reviewed and debated (p293; emphasis added).
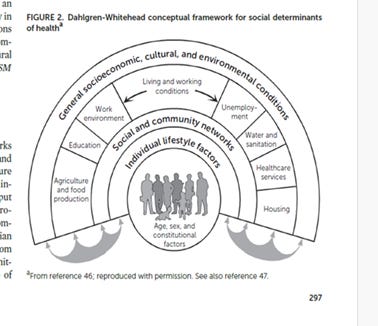
Finally, there is the ancient question of how to take account of “neurobiological, developmental, experiential, socioeconomic, cultural, and environmental factors” in the development of mental disorder: “This can be accomplished by including descriptive language but also by finding a pragmatic way to integrate biomarkers and other biological factors, recognizing that it is very early days for most of these” (p296; emphasis added). One possible means of integrating them is shown in a diagram:
All of this sounds terribly impressive, as it is intended to do, because it conceals an almost frightening level of ignorance about their subject matter. In a few words, they don’t know what they’re talking about but they don’t want you to know that. It’s full of little ploys to mislead people, including some fairly sophisticated readers. For example: “... we still do not fully understand the etiology of disorders ...” That actually means: “We haven’t got a clue.”
Continuing, we are told: “DSM is not based on empirical science...” but experts look at the data and debate it. All very well, but remember that people see only what they want to see. If I look at a case of depression, I see a seriously anxious personality based in a long history of emotional deprivation and abuse. Their experts look at the same case and see a biological specimen. The notion that experts are objective and unbiased is simply false, as astrophysicist Carl Sagan noted: “Evidence that contradicts the ruling belief system is held to extraordinary standards, while evidence that entrenches it is uncritically accepted.” This is absolutely fundamental, how can they be so easily fooled? Because their minds are made up. Andrew Scull recounts how two psychoanalysts were recruited to the DSM-III committee [5, chap 18]. After months of trying to get alternative views accepted, they resigned.
The “arbitrary nature of categorical boundaries.” Again, this is fundamental, you can’t write a description of mental disorder if there’s no formal way of deciding what is or isn’t mental disorder. They poked around with a dimensional model for personality disorders in DSM5 but soon gave up as it quickly unravelled the entire DSM edifice. You can’t build one part of your diagnostic system based on the idea that there are hard cut-off points in the data, and the other part on the idea that there are no cut-offs, that normality spreads smoothly across to abnormal and it is entirely a matter of taste where you put the boundary. That’s not science, sorry.
“Another important limitation of DSM is the lack of inclusion of candidate or actual biomarkers or biological processes.” Before you start spending money on the search for biomarkers, can we just sort out the question of whether there are any? If mental trouble is wholly a matter of psychology, as the biocognitive model says it is, then searching for “biomarkers” is a waste of jolly time and money (usually known as a WOFTAM but this is a polite file). The decision that it is biological is driven by a misunderstanding of what positivist science is about, ably amplified by the American insurance industry and the international drug industry. Plus academics who mistake clouds of dust for a passing bandwagon. And Alzheimer’s Disease is not a psychiatric condition anyway. Sure, there may be psychiatric complications but that happens with broken legs as well.
“Although there is broad agreement in the field that (mental) disorders arise from the interplay of neurobiological, developmental, experiential, socioeconomic, cultural, and environmental factors, knowledge about precisely how these factors interact is still evolving.” A good starting point would be a formal theory of mind, leading to a model of mental disorder, such as the biocognitive model. Absent that, the diagram they offered (above) is just self-righteous drivel. All the factors it shows simply swirl around in space, unconnected and mostly ignored. As for the expression “precisely how these factors interact,” that’s a euphemism for “no jolly idea,” usually abbreviated to NFI. You and I know that but politicians, bureaucrats, lawyers and other pond life are led astray by this high-sounding talk, they think it means (as they are intended to think) “built on a solid foundation of science, on the verge of major breakthroughs.”
The old “reliability vs validity” argument will never be settled without a formal model of mental disorder but they showed a modicum of insight by raising the question of reification. This means turning an abstract concept into a real entity. Is schizophrenia a real thing or not? What about ADHD, is it real or just a faddish label applied to children who don’t fit the mould? In fact, reification is inevitable. If you’re not sure whether something is real or just an artefact, then the definition becomes circular: “He has ADHD because he has these symptoms, and his ADHD causes the symptoms.” I once asked a 43yo woman with a long history of treatment for depression why she was feeling sad. “Oh, she replied, “it’s my depression, it always does it.” We went through her history and I finally said: “Well, the reason all those antidepressants haven’t worked is because the real problem since childhood has been your severe anxiety state.” “Anxiety?” she shrieked, clutching her head. “Oh no, that’s terrifying.” Indeed it is, and when you get trapped in a self-reinforcing anxiety state, life can get pretty depressing, but there are no biomarkers as it’s entirely psychological. All of this biology-talk is deceitful, but it’s the worst sort of deceit, self-deceit. Carl Sagan again:
One of the saddest lessons of history is this: if we’ve been bamboozled long enough, we tend to reject any evidence of the bamboozle. We’re no longer interested in finding out the truth. The bamboozle has captured us. It’s simply too painful to acknowledge, even to ourselves, that we’ve been taken. Once you give a charlatan power over you, you almost never get it back. So the old bamboozles tend to persist as the new ones rise.
Is psychiatry just charlatanism? The burden of proof rests on those who say it’s not, the nul hypothesis has to be that it doesn’t reach the high standards of science. I agree, I say it doesn’t, and this paper by a committee of worthies published in a prestigious journal is proof. Trouble is, we now have two generations of psychiatrists who have been force-fed on DSM and are now indoctrinated in this bizarre system. They are perfectly comfortable with the idea that psychiatry doesn’t need a theory of mind or model of mental disorder, or theory of personality or model of personality disorder. For them, in their placid, self-assured echo chamber, the rigid descriptions in DSM tell us all we need to know about mental disorder, especially as their drugs will clean up any rough edges.
Plus ça change, plus c’est la même chose.
References:
1. Guze SB. Biological psychiatry: is there any other kind? Psychological Medicine, 1989; 19: 315-323.
2. McLaren N (2007). The categorical system of diagnosis: Personality Disorder. Chapter 8 in Humanizing Madness: Psychiatry and the Cognitive Neurosciences.; Ann Arbor, Mi.: Future Psychiatry Press.
3. Horwitz AV, Wakefield JC (2007). The Loss of Sadness: how psychiatry transformed normal sorrow into Depressive Disorder. New York: Oxford University Press.
4. Oquendo MA et al (2026). Initial Strategy for the Future of DSM. Am J Psychiat 183:5, 292-300.
5. Scull A (2022) Desperate Remedies: Psychiatry and the mysteries of mental illness. London: Penguin.
****
My critical works are best approached in this order:
The case against mainstream psychiatry:
McLaren N (2024). Theories in Psychiatry: building a post-positivist psychiatry. Ann Arbor, MI: Future Psychiatry Press. Amazon (this also covers a range of modern philosophers, showing that their work cannot be extended to account for mental disorder).
Development and justification of the biocognitive model:
McLaren N (2021): Natural Dualism and Mental Disorder: The biocognitive model for psychiatry. London, Routledge. At Amazon.
Clinical application of the biocognitive model:
McLaren N (2018). Anxiety: The Inside Story. Ann Arbor, MI: Future Psychiatry Press. At Amazon.
Testing the biocognitive model in an unrelated field:
McLaren N (2023): Narcisso-Fascism: The psychopathology of right wing extremism. Ann Arbor, MI: Future Psychiatry Press. At Amazon.
The whole of this work is copyright but may be copied or retransmitted provided the author is acknowledged.